Cardia, pericardium, epicardium, myocardium, endocardium
Medical: Cor
English: heart

The heart (cor) is a muscular hollow organ that is embedded in the middle membrane (mediastinum) between the two lungs (see also lungs), protected from the outside by the bony chest (thorax). It works like a pump that transports the blood through both the small and large circulation in the body.
Read more on the subject: Task of the heart

You can find an overview of all Dr-Gumpert images at: medical illustrations
$config[ads_text1] not found
The shape of the heart does not correspond to the symbol used in everyday life. It is more like a cone, with the apex cordis pointing to the left - front - below, the base of the heart (base cordis) pointing to the right - above - back.
An adult's healthy heart has a volume that is slightly larger than its own fist (500-800ml) and weighs between 250-350g.
At 500 gr, the so-called critical heart weight is reached, since from this size a pathological enlargement of the heart (hypertrophy) occurs.
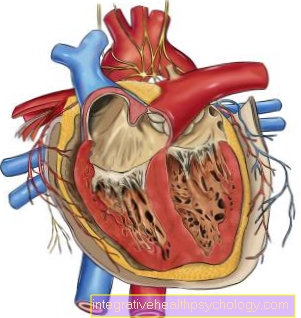
From a tissue perspective (microscopic), the heart can be divided into individual functional layers.
Seen from the outside in, these are:
The heart is enclosed by a tough connective tissue sac (Pericardium), the one with the diaphragm (Diaphragm) has grown together. It follows that the exact position of the heart in the body depends on the breathing.
The pericardium forms a tight covering around the heart, which primarily provides mechanical strength. Starting from the pericardium, the next layer is also smooth, but clearly thinner and more delicate (epicardium), which includes the muscles and the attachments of the large blood vessels supplying the heart (coronary vessels, vasa privata, coronary vessels). Coarse unevenness through the vessels is evened out by a layer of fat.
The next and by far the thickest layer is the heart muscles (Myocardium). It is the real engine of the cardiovascular system. The muscles are only separated from the blood by a very thin layer of cells (Endocardium), which is very smooth on the side facing the cavities (lumens, heart cavities).
The heart has four cavities, one each right and a left Forecourt (Atrium) as well as a right and a left ventricle (Ventricle). The cavities are separated from one another by muscles. There is a Atrial septum (with the foramen ovale closed after birth), an atrial-ventricular septum and the Chamber partition between the two Chambers of the heart.
As in the veins of the body, the direction of blood flow in the heart is through the heart valves (Leaflet flaps, between atrium and chamber, and pocket flaps, between chamber and outflow path)
The used (low-oxygen) venous blood from the large body circulation reaches the upper and lower Vena cava (superior vena cava and inferior vena cava) into the right atrium, then through the right leaflet valve (tricuspid valve = Valvula atrioventricularis dexter) into the right ventricle and is from here via the right pocket valve (Pulmonary valve) in the Pulmonary circulation (small circuit) pumped. After it has taken up oxygen there, it returns to the heart in the left atrium. From there it takes the same route as on the right, only accordingly through the left flaps: through the left leaflet valve (mitral valve = Valvula atrioventricularis sinister) into the left ventricle, and then through the Aortic valve in the great body circulation to be pumped.
$config[ads_text3] not found
What applies to all valves is that they only allow blood to flow in one direction. The sail flaps are called sail flaps because they are shaped like the sails of a sailing boat and are attached to the ventricular muscles by tendons (papillary muscles, chordae tendinae) - so they cannot swing too far back. The pocket flaps work a little differently: They are built in such a way that when the blood flow is reversed, they are pressed against each other and therefore cannot penetrate through. All four heart valves lie in one spatial plane.


The Endocardium is a flat, unicellular layer that separates the ventricular muscles from the blood. Functionally it corresponds to the inner lining of the blood vessels (EndotheliumIts task of preventing the formation of a blood clot (thrombus) is ensured by its special, smooth surface and by the production of anticoagulant substances (nitric oxide (NO), prostacyclin).
$config[ads_text4] not foundThe Myocardium (Heart muscles) is the drive for blood flow (convection) throughout the body. The muscle cells are kind of a mix of smooth and striated Musculature.
They have the same mobile protein complexes (sarcomeres from actin, myosin and titin) as they do Musculature of the musculoskeletal system (striated muscles) and therefore also the same mechanism to control a contraction of the protein complexes. This mechanism consists of other proteins (troponins), which can take on different structures and which, depending on the state, allow or prevent the individual building blocks of the protein complex from working together / contracting.
What the Heart muscle cells of the Skeletal muscle cells differs, the arrangement of the individual cells in all directions of the three-dimensional space and their centrally located nucleus - both characteristics of the smooth muscles (viscera). The muscle cells are connected to one another via firm cell-cell connections (desmosomes).
There is also another type of cell-cell connection (gap junction) that fulfills an electrical function by connecting the individual cells to one another in an electrically conductive manner. This is why one speaks of a functional syncytium (cell association without cell boundaries).
The muscle layer is not the same thickness in the whole heart. The thickness of the muscle layer ranges from 2-3 mm in the right atrium to 12 mm in the left ventricle. These differences are an expression of the different pressures that prevail in the individual heart cavities.
There are other specialized cells called myoendocrine cells in the wall of the right atrium. By their origin they are muscle cells, but they are the Hormones ANP (atrial natriuretic peptide) and BNP (brain natriuretic peptide). They are formed when excess blood is measured in the atrium. Their effect lies in an increased excretion of fluids (diuresis) by the kidneyto prevent such an excess of blood.
The muscle cells of the heart begin their work before birth and beat for a lifetime. They cannot be replaced by new cells and still have to do something unimaginable: 30 million heartbeats per year! They need a lot of energy for that. The heart muscle cells are the cells in the body that consume the most oxygen and have most of the "power plants" for providing energy (mitochondria).Heart attack, angina pectoris) are very quickly threatened with life.
In evolutionary terms, the epicardium and pericardium are the two leaves of the classic serous organ sheath. The visceral leaf is the epicardium, the parietal leaf is the pericardium. At the border between the two leaves they are very smooth and separated by a very narrow, fluid-filled cavity. They enable the heart to move with almost no friction. Furthermore, the outer (parietal) sheet (pericardium) gives with its taut connective tissue mechanical stability to the heart.

The heart is supplied with oxygen by its own vascular system (coronary arteries).
The vessels are located within the pericardium. The two cardiac arteries (arteria coronaria dextra and sinistra) both arise directly from the initial part of the aorta, a few millimeters behind the Aortic valve. The left cardiac artery (LCA = Left coronary artery) runs forward at the level of the atrium-ventricular boundary and then divides into a descending branch (Ramus interventricularis anterior (LAD = Left anterior descending) and a more horizontal branch (RCX = Ramus circumflexus)). The right coronary artery (RCA = Right coronary artery) is the smaller of the two cardiac arteries and runs backwards, also at the level of the atrial-ventricular border. With the sinus and AV nodes, it supplies the two crucial stations of excitation formation.
Of all these arteries named here, smaller branches extend into the muscles to be supplied in the direction of the heart cavities. Only the innermost layers of the myocardium are supplied directly from the heart cavities by diffusion (uptake of blood components due to differences in concentration). Due to the high pressure that is generated in the left ventricle in particular during systole (> 120 mmHg), the vessels in systole are squeezed shut. It follows from this that the supplying blood flow only progresses in diastole. The problem that arises from the diastolic blood flow: With increased Heart rate the diastole is shortened disproportionately - the time for an oxygen supply as well. However, the increased cardiac output increases the need for oxygen. This is a contradiction that can be dangerous to the sick heart.
There are basically two ways for the venous return flow: The main way collects the blood in one Cardiac vein (Sinus coronarius) and flows into the right atrium, as does the rest of the body's used up blood. A secondary route for the venous blood are the smallest veins that flow directly into all four heart cavities. It must be added here that the high pressure during a heart contraction literally squeezes the veins - the return flow works without problems in almost all hearts.
Further information is also available under our topic: Vascular supply from the heart












