Patellar fracture, transverse patella fracture, longitudinal patellar fracture, longitudinal patellar fracture, transverse patella fracture, kneecap arthrosis, retropatelar arthrosis, fracture of the kneecap, fracture of the patella, knee
When the kneecap breaks, the kneecap fractures into several parts. This can result in longitudinal, transverse or mixed breaks. The treatment of the kneecap fracture depends crucially on the type of fracture.
Patellar fractures make up about 1% of all fractures.

In most cases, it is a fall on the bent knee joint. The force of the direct impact breaks the kneecap into two or more fragments.
$config[ads_text1] not found
In traffic accidents, a patellar fracture can also occur when the bent knee joint is struck. These violations are also known as "dashboard violations".
In exceptional cases, sudden flexion of the muscularly maximally stretched knee joint can lead to a fracture of the kneecap.
Another rare cause is the dislocation of the kneecap (patellar luxation), which can lead to lateral shearing of the kneecap.
Appointment with a knee specialist?
Who am I?
My name is dr. Nicolas Gumpert. I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
The knee joint is one of the joints with the greatest stress.
Therefore, the treatment of the knee joint (e.g. meniscus tear, cartilage damage, cruciate ligament damage, runner's knee, etc.) requires a lot of experience.
I treat a wide variety of knee diseases in a conservative way.
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
Further information about myself can be found at Dr. Nicolas Gumpert
Basically one differentiates Transverse breaks, so-called transverse fractures of Longitudinal breaks (Longitudinal fractures) that break the axis of the leg.
Furthermore, the number of fragments is included in the classification. The position of the fragments against one another is also examined, so that one speaks of unshifted (undisplaced) and shifted (dislocated) fractions.
Classification of AO (Working group for osteosynthesis)
In addition to the well-known AO classification, there are many other classifications that we do not want to go into at this point.
$config[ads_text2] not found
$config[ads_text3] not found

Transverse fracture - longitudinal fracture - multi-fragment fracture
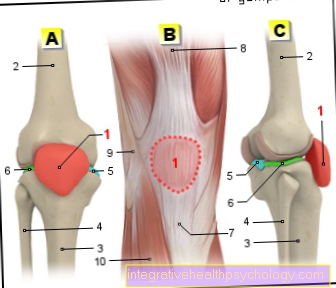
You can find an overview of all Dr-Gumpert images at: medical illustrations
A kneecap / patellar fracture causes pain over the kneecap. It is typical that the lower leg cannot be actively stretched or the knee joint cannot be kept stretched because the anterior thigh muscles (quadriceps femoris muscles) can transfer the force to the lower leg via the kneecap.
The fracture of the kneecap results in a bruise / hematoma. The bruise shows up under the skin as a "bruise". The bleeding into the knee joint appears as a knee joint effusion (intra-articular effusion, bloody effusion = hemarthrosis).
$config[ads_text4] not found
As the cause is often falls on the kneecap, abrasions are often found in this area.
Depending on how severe the injury is, the symptoms of a fractured kneecap can vary in intensity.
In any case, a thorough diagnosis should be carried out, since the extent of the symptoms does not always necessarily go hand in hand with the objective finding. Just because pain may not be very pronounced, serious damage and accompanying complications can nonetheless occur, which should not be overlooked due to the high pain threshold of a person affected.
In the case of a fractured kneecap (Patellar fracture) It comes to typical symptoms:
The diagnosis of a knee fracture is usually made by a X-ray image posed.
The knee joint is x-rayed in two, if necessary in three planes.
Often this means that the extent of the injury cannot be adequately represented and it becomes a supplement Computed tomography (CT) made. Computed tomography can also show microfractures that are not visible in the X-ray image.
As a further sensible measure, the doctor is available Magnetic resonance imaging (MRI) of the knee available. The cartilage damage behind the kneecap can be better assessed in the MRI image of the knee. By breaking the bone, the cartilage of the posterior kneecap also breaks. Since the cartilage cannot be shown in the X-ray image or in the CT, the MRI of the knee is a valuable source of information here.
A possible cause that causes comparable damage is a rupture of the kneecap tendon (patellar tendon rupture) with the following elevation of the kneecap or a tear of the quadriceps tendon with a depression of the kneecap.
Constitutional abnormalities are two-part (patella bipartita) or three-part (patella tripartita) kneecaps. Usually the extra piece of bone is in the upper outer quadrant of the kneecap. Since this anomaly is often bilateral, an x-ray of the kneecap can be helpful.
Read more on the subject at: Bipartite patella

Fractured kneecap - the lower third of the kneecap is broken.
This fracture is difficult to treat surgically, since screws, wires, etc. can be placed in the smaller, lower fragment without further breaking the fragment.

X-ray image of the knee joint:
Condition after refixation with wire cerclage
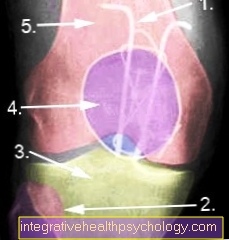
X-ray image of the knee joint from the front:
Figure 8 harness and equatorial cerclage
The kneecap fracture (Patellar fracture) can be treated conservatively and surgically. Longitudinal kneecap fractures and undisplaced fractures can be treated conservatively, all other types of fracture should be treated surgically.
In the therapy of the kneecap, a knee orthosis is prescribed with restricted mobility. The flexion should not be more than 60 ° within the first three weeks and not more than 90 ° up to the sixth week.
The knee joint should only be loaded with 20 kg within the first three weeks and loaded to full load up to the 6th week. Until the actual full load is reached, thrombosis prophylaxis, e.g. be carried out with low molecular weight heparin.
This post-treatment scheme must be deviated from in individual cases.
Kneecap fractures with displaced fractures and a step formation of more than 2 mm and a divergence of the fracture fragments of more than 3 mm should be treated surgically. In particular, cross-fragment and multiple-fragment breaks require surgical therapy.
The decision about the type of surgical treatment must be adapted to the individual findings.
So-called tension belt osteosynthesis, cerclages and screwing of the fracture are available for surgical treatment.
$config[ads_text2] not found
Tension bands are often used for transverse fractures with few fragments and are therefore the most common type of restoration. Here, two wires are brought through both fragments along the length of the kneecap. A wire loop in the shape of an 8 is placed around these two wires. By pulling these wire loops, the fragments are put back together and can heal.
In addition, the fracture can be secured with a so-called equatorial cerclage, especially in the case of multiple fragment fractures.
In the case of a fracture of the kneecap in the form of a transverse fracture with a few fragments, a screw connection can also be used as an alternative.
In hopeless cases, in which no gradual restoration is possible, the complete removal of the kneecap must be considered (Patellectomy), since otherwise a symptom-causing osteoarthritis develops in the short term.
The Knee joint should only be flexed a maximum of 60 ° within the first three weeks after the kneecap surgery and a maximum of 90 ° up to the 6th week.
The load on the operated leg should not be more than 20 kg at the beginning and should be increased to full load by the end of the sixth week.
This post-treatment scheme must be deviated from in individual cases.
X-ray controls should take place after 2, 4 and 6 weeks.
The smaller the damage to the kneecap, the better the long-term prognosis. Approx. 1/3 of all patients with a fracture of the kneecap have to reckon with stress-dependent or permanent pain despite optimally treated patella fractures.
Particularly in the case of multi-fragment fractures, fragmentary fractures and fractures that can only be reassembled with step formation, the risk of permanent complaints is increased.
The incidence of kneecap arthrosis (retropatellar arthrosis) is significantly increased after a patellar fracture.
There is also the risk of joint scarring (Arthrofibrosis).
If the kneecap is treated surgically, it usually takes about 6 weeks until the fracture has healed to such an extent that a full load is possible.
Of course, the regeneration time varies from patient to patient, so that the 6 weeks should only be seen as a rough guide.
It happens time and again, for example, that patients do not have symptoms beyond the 6 weeks.In some cases, it takes several years for the patient to heal completely; in exceptional cases, patients after a fractured kneecap have to struggle with kneecap complaints for life.
In order to positively influence the healing time of the kneecap, the surgical treatment is followed by rehab (rehabilitation) on.
Rehabilitation, among others Guided by physiotherapists and sports therapists, it includes exercises to strengthen the surrounding leg muscles and stabilize the leg axis in the case of a fracture of the kneecap and coordination exercises and the wearing of movement splints on the other.
The duration can go beyond the hospital stay of several days up to a week, as required. In the form of the smallest training units, e.g. moving your feet, the rehab begins on the first day after the operation.
The duration of the rehab depends on factors such as age, the severity of the kneecap and possible previous illnesses. Generally, there is no prescribed length of stay, but discharge is usually planned on the 2nd day after the operation.
If complications occurred during the operation or if wound healing was difficult, it is at the discretion of the attending physician to postpone the discharge date for a few more days.
The incapacity for work after a kneecap fracture is approximately 6 weeks. Depending on the activity to be performed, the incapacity for work can be longer, e.g. if work has to be carried out on the knees or if the knee is generally extremely stressful.