Neck school group concept
information
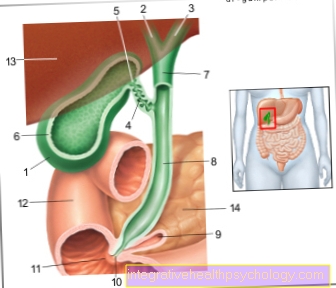
At the beginning of the neck school, information is provided about the individual problems of the participants (useful in a one-on-one conversation in advance), background knowledge about anatomical basics, pathological muscle activity, stressors, chronification mechanisms, neck-friendly work, recommended sports.
Consistent participation:
The participants are encouraged to take part in the group program continuously and consistently, otherwise the chances of success decrease significantly. In each exercise unit, known exercises are repeated and increased, new exercises are added, information and assistance are given. Through constant repetitions, the movement sequences are automated, unfavorable movement and tension patterns dissolve.
Instruction, support and correction by the instructor are useful and necessary over a period of at least 10 weeks in order to learn the exercises and to be able to implement them correctly in everyday life.

Active participation:
Active participation according to the therapist's instructions during the group lesson and continuing the exercise program at least 1-2 times / week at home in addition to group participation is a prerequisite for the success of the treatment.
Moving and exercising despite and because of complaints
The unusual activation of tense, shortened or “weak muscle groups” can lead to unpleasant feelings of tension and sore muscles. There may even be an increase in pain in the neck and head area or dizziness. The participants must be informed in advance about these "undesirable reactions" in order to be able to deal adequately with the increased pain situation. Otherwise there is a risk that those affected will drop out of the neck school.
In any case, the exercises should be continued, even if the pain increases. With the help of the physiotherapist, the execution of the exercise, the range of motion or the intensity can be changed. Limits, with the aim of expanding them over time, must be respected. Under certain circumstances, pain medication can even temporarily allow the program to continue. When the participants have learned to assess the situation and react appropriately, mechanisms of self-efficacy are stimulated and self-confidence is strengthened.
As the symptoms improve and the negative reactions to stress decrease, the motivation of those affected to stick to the program increases.
FEAR OF PAIN-INDUCING ACTIVITIES DECREASE!
Appointment with a back specialist?

I would be happy to advise you!
Who am I?
My name is dr. Nicolas Gumpert. I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
The spine is difficult to treat. On the one hand it is exposed to high mechanical loads, on the other hand it has great mobility.
The treatment of the spine (e.g. herniated disc, facet syndrome, foramen stenosis, etc.) therefore requires a lot of experience.
I focus on a wide variety of diseases of the spine.
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- Lumedis - your orthopedic surgeon
Kaiserstrasse 14
60311 Frankfurt am Main
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
Further information about myself can be found at Dr. Nicolas Gumpert
Continue the program at home, check-up appointment
The group participants should continue the program learned in the group over the 10 weeks and the self-help strategies for pain or dizziness for at least 4-6 weeks at home with a frequency of 3-4 exercise units / week of 20 minutes. The exercises learned and neck-friendly working behavior must be integrated into everyday life. A fixed exercise date is recommended, e.g. in the morning before a shower or in the evening with the news. Regular practice of a neck / back-friendly sport such as Nordic walking or backstroke swimming can significantly support the healing success.
After that, another check-up appointment should take place to check the success of the neck school with the prescribing doctor using the physiotherapeutic therapy report. This check-up appointment should include a conversation and an examination of the results achieved in terms of pain behavior, mobility and resilience.
Depending on the outcome of the treatment, the further procedure will be discussed with the doctor or the physiotherapist.
- If there is no pain (very often), the program can be continued in a “slimmed-down” form and maintained over the long term. A study has shown that the freedom from pain achieved lasts only with continuous training.
- If there is improvement (less often), individual physiotherapeutic therapy or other therapeutic measures can be carried out in addition to continuing the program if functional complaints are still present. The aim should be independence and independence in dealing with the pain.
- If the pain condition remains unchanged (individual cases), the doctor should re-diagnose and carry out a modified pain therapy. Perhaps taking a closer look at the psychosocial factors that maintain the pain can bring about further therapeutic success.
Active exercise program of the neck school
- Warm up exercises
important: high fun factor, partner exercises, coordination exercises
- Body awareness training
The group participants learn the different possibilities of movement of the cervical spine and the Shoulder girdle and know the link between breathing and movement. By drawing attention to the muscles, you will be able to feel the difference between tense and relaxed muscles. Especially that Perceiving relaxation is an important prerequisite for the correct execution of the exercise program and the later transfer of what has been learned into everyday life.
Perception training also includes learning the local stabilization exercises.
- Strengthening program
Strength / muscle building has been shown to have the highest treatment effectiveness in terms of pain relief compared to a general fitness or exercise program. In one study, 73% of the participants who had carried out special strength training for the neck, neck and shoulder muscles 3 times a week for a year had a clear reduction in symptoms.
The aim of the strengthening program is to improve the stability of the cervical spine and relieve the strain on the shoulder muscles, which are usually very tense (shoulder lifter). In the foreground is next to Training of the deep, short neck muscles Strengthening the flexion, extension and rotation muscles of the cervical spine, the shoulder blade stabilizers and the back extension muscles. Small devices such as Theraband, weight cuffs or small dumbbells can be used to intensify the training stimulus.
The use of special strength equipment for training the neck - and Shoulder muscles Unfortunately, it often turns out to be a pain intensifier due to the excessive training stimulus in relation to the increased sensitivity of those affected. In addition, the participants cannot carry out this training measure independently at home.
Exercise examples for strengthening the neck muscles
The selection, duration and number of repetitions of the exercises depend on the individual pain, strength and movement findings!
The aim for strength endurance training is a holding time of 7-10 seconds and 3 repetition series of 10 exercises.
Important: Pay attention to calm, even breathing during the exercises!
A mirror for self-control can be useful for exercises while sitting.
Caution: When exercising with dumbbells or weight cuffs, the weights should not be lifted with an extended arm from bottom to top over a 90 ° arm-torso angle.
Exercise 1
Starting position
upright seat on the stool
Exercise execution
the chin is pulled back, the back of the head pushed out, the cervical spine describes a small flexion movement


exercise 2

Starting position
upright seat on the stool
Exercise execution
the head is moved backwards while maintaining the flexion
Important: the chin should not point towards the ceiling!
Exercise 3

Starting position
upright seat on the stool
Exercise execution
Both shoulders are moved from the top front to the back, the shoulder blades are pulled back and down towards the trouser pockets and held
Exercise 4

Starting position
upright seat on the stool
Exercise execution
the head is pressed sideways against the hand and held
Execution of the exercise: the head is turned right / left against the hand and held
Exercise 5
Starting position
Quadruped, knees and hands are at right angles under the shoulder girdle and pelvic girdle, the back is flat (pull the navel towards the spine)
Exercise execution
The head is moved down in the direction of flexion, then up in the direction of extension

Exercise 6

Starting position
Prone position on the mat: forehead covered with a small towel, navel drawn towards the spine
Exercise execution
the fingertips are on the back of the head, the chin is pulled towards the navel, the head is raised, the back of the head is pressed against the fingertips and held
Exercise 7

Starting position
Lie on your back on the mat: the legs are raised, the arms are next to the body, the head if possible flat on the mat
Exercise execution
the chin is pulled towards the breastbone, the back of the head is raised approx. 1 cm from the floor
variation
Look over the right / left chest, then again lift the back of the head approx. 1 cm from the floor
Exercise 8
Starting position
Sit on the mat with your legs raised
Exercise execution
Both arms are stretched forward, the chin is drawn towards the sternum, the upper body is slowly moved towards the supine position to the point at which it is still possible to sit up and back up.
The instructing physiotherapist must address the individual performance level of the group participants and take into account differentiated exercise information. The aim is for all group participants to be able to perform the exercises correctly and to continue the exercise program at home without control.
The exercise intensity and thereby the training stimulus are increased in the course of the 10 exercise units in terms of execution, holding time, force requirement, number of repetitions, etc.
During the 10 exercise units, an increase in performance in terms of coordination and muscle strength should be achieved for all course participants within their individual load limits.

Exercise examples for posture training, mobilization, stretching, relaxation
Learning the correct posture is a very important part of the exercise program right from the start, especially for those affected who work in a seated workplace. Due to the hunched back caused by a lack of muscle activity, the cervical spine has to perform a compensatory movement forwards (reinforcement of the natural curvature forwards = lordosis), otherwise the line of sight e.g. towards the screen is no longer possible. As a result, the skull slides slightly forward on the upper cervical vertebra, which can lead to irritation in the head joints and increased pressure on the small vertebral joints. The slackening of the anterior neck flexor muscles results in muscle imbalances, tension in the neck and shoulder muscles, neck headaches and dizziness.
Exercise posture training:
Starting position: sitting on a stool
Exercise execution:
lift the sternum, push the back of the head out towards the ceiling, pull the navel towards the spine, pull the shoulder blades back and down towards the pockets.
The establishment of an ergonomic workstation to support the upright posture and to relieve the neck, best as a preventive measure, is essential.
Mobilization exercises:
The aim of the mobilization exercises is to improve mobility in the cervical spine and to break up changed movement patterns. Example: Patients who are careful not only turn their heads when they look around, but also turn their entire thoracic spine. The fear of movement is reduced by the targeted exercises, the extended range of movement can be perceived as a pleasant relief for everyday movements.
Exercise example mobilization:
Starting position: sitting upright on the stool
Execution of the exercise: the head is turned to the side until the pain-free end position (looking around the shoulder), with the help of a long exhalation one tries to move the head further in the direction of rotation over 3 breathing phases until the pain threshold is reached Head slowly moved back to the middle position.
Important: the shoulders and knees are facing forward during the exercise
The same exercise sequence can also be performed in the flexion or side-bending motion of the cervical spine.
Exercise example stretching

Starting position
upright seat in front of the mirror
Exercise execution
the head is tilted to the right / left side towards the ear and turned to the opposite hip. One hand grabs over the head and carefully supports the tilting movement, the other hand pushes the palm of the hand sideways to the floor. A pulling sensation develops on the shoulder side where the hand pushes towards the floor. (Muscle stretching)
Relaxation exercises:
1. Whole body relaxation:
Autogenic training - physical relaxation through mental imagination or the Relaxation exercises according to Jacobsenwhere relaxation is perceived and learned by tensing the various muscle groups of the whole body beforehand.
2. Targeted relaxation of individual muscle groups:
Exercise example for targeted relaxation of the shoulder jack:
Starting position: Sit upright on the stool
Exercise execution: Both shoulders are pulled into the tense position towards the ears and held there until the Shoulders acheThen, with a deep exhalation, the shoulders are deliberately dropped. You can take a light dumbbell or an adequate weight in your hands for support.
This exercise should be repeated until the shoulders feel relaxed and warm.
The aim of the exercise is that the patient perceives his tense shoulder position in everyday life - constant pulling of the shoulders - and learns to correct independently.
Mediation of self-help strategies
There are various options for self-help in the case of pain intensification, regardless of whether it was caused by the exercises or during stressful everyday activities:
- Trigger point treatment see below
- warmth
- Treatment with the tens device
- Stretching exercises
- Possibly medication
- Tape
Examples of trigger point treatment:
Transverse expansion:
Starting position: upright seat on the stool
Exercise execution: one arm is turned out next to the body. The other hand grabs the upper part of the shoulder muscle over the shoulder in question. With the exhalation, the muscle is pulled forward and held for a few seconds. In this way, the muscle is stretched and relaxed across its course. This exercise should be repeated several times, preferably several times a day in the case of severe tension complaints on the shoulder.
Trigger point massage:
Starting position: Lie on your back, small pillow, knee roll if necessary
Exercise execution: 2 tennis balls are placed under the right and left shoulder on the pain points of the large shoulder muscle. The head is relaxed on a small pillow. By slowly rolling the head from one side to the other, the muscles are massaged by the tennis balls.
Trigger point massage as a partner exercise:
Starting position: upright seat, the partner stands behind it:
Exercise execution: The partner massages the pain points on the right and left of the spine (from top to bottom) and on the shoulder muscles (from inside to outside) with two hedgehog balls using small, circular movements. At the beginning only slight pressure should be exerted, later pressure increase is possible. After massaging, feel the relaxation of the worked areas.