This topic mainly deals with the psychological aspects from being overweight. Permanent weight reduction can only be achieved if the mechanisms that lead to obesity are understood.
Medical: obesity
Overweight, fat, fat, fat, stout, corpulent, full figured, plump, obesity per magna, obesity, ideal weight, normal weight, underweight
English: overweight
The term Obesity (Obesity) describes a condition in which a person is more weight than the normal value (normal weight), which is considered optimal for his body size, and is thereby exposed to increased health risks.
The degree of obesity in need of treatment (overweight) is calculated using the so-called Body mass index.
You can find more information about the calculation at: Body mass index.
$config[ads_text1] not found
General classification of the body mass index (BMI = kg (body weight) / (height in) m2)
In most cases there is only one BMI greater than 30 need treatment. Of course, the level of the treatment is not the only factor BMI decisive, but in particular the distribution of the fat. E.g. known that with the fat distribution in the abdomen, which is typical for men, there is a much higher risk of myocardial infarction than with the hip fat accumulation which is more common in women.
Not to be forgotten, of course, are psychological stress, as well as high psychological stress, from which, regardless of BMI (Body Mass Index) a need for treatment can arise.

$config[ads_text2] not found
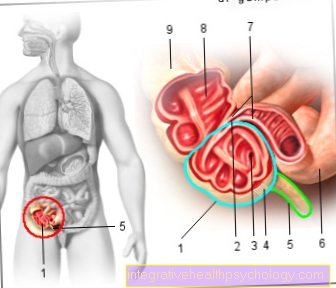
Typical illnesses caused or partly caused by obesity:
Obesity is associated with a variety of direct and indirect health risks. The following are the most important:
Also there are related to Obesity / overweight clear for the sick “Psychosocial” consequences. This describes the worries that arise when dealing with the environment.
Often times, self-esteem and life satisfaction are severely impaired. Anxiety disorders and depressive moods are not uncommon.
Please also read our topic on this Consequences of being overweight.
Occurrence in the population
About every 5th adult and every 20th adolescent in Germany suffers from obesity that requires treatment (overweight).
The likelihood of becoming overweight clearly increases with age. Women in particular are at risk as they get older.

In addition to determining the BMI (Body mass index) and the distribution of fat, medical laboratory tests are necessary in order to assess the risk of the diseases mentioned above.
Furthermore, a so-called "Weight curve" to be created. The patient draws the previous course of his weight in this and discusses with a doctor / therapist whether he can assign certain fluctuations in weight to certain life events. In this context, the patient should also create a desired curve from which his target weight can be read.
Furthermore, so-called. Food diaries proven, in which all food and drinks that the patient consumes are noted for a week.
This tool is particularly important to any Binge eating disorder or other unfavorable eating behavior (e.g. frequent consumption of sugary lemonade or particularly high-fat food, etc.).
$config[ads_text2] not found
In contrast to the popular opinion that obese / overweight patients simply eat too much, science in recent years has shown that various influencing factors play a role in the development of overweight (obesity).
The modern therapeutic approach to treating the Obesity must take into account today's knowledge of this disorder. It just isn't enough to stop eating an obese patient and scare them with stories of high blood pressure and heart attacks. Today's therapy should be carried out in different stages, which ideally build on one another.
$config[ads_text4] not foundMost obese (overweight) people carry around with them a picture of themselves and their disorder, in which they usually see themselves as the culprit for their disorder.
As mentioned above, however, this is by no means fully applicable. Of course, it is by no means beneficial for a patient to eat exclusively junk food and avoid any kind of exercise, but it is just as wrong to label an overweight person as lazy wolverine per se. The truth lies (as is so often the case in our beautiful world, which is neither entirely black nor entirely white) in the middle.
The therapist's task is to explain the whole range of causes to the patient in order to work on his attitude towards himself. The message here should be that much of what constitutes obesity (overweight) is through no fault of our own, but that we do not simply have to accept this fate.
Most obese patients who come into such therapy have already had a large number of failed diets and have therefore often left the mark of failure on themselves. The honest and scientific explanation of the disorder should now lead to a rethink and give a new motivation boost.
If the patient should have developed a motivation for a therapy through this first step, the next step is to determine the goals of the therapy. Unfortunately, in many cases, motivation or over-motivation leads to the motivated person setting unachievable goals at which he will almost certainly fail. (E.g. the weight reduction from 120 to 70 kg within half a year)
Such a failure can destroy the newly created motivation and ultimately lead to weight gain (black and white thinking) by completely giving up the attempt to lose weight.
Regarding the target weight, there are guidelines that assume that it makes sense to initially reduce the starting weight by around 15%.
As already mentioned, it is usually only annoying to forbid a person to eat.
For this reason, it is important not to consider the food itself, but its composition in the therapy. In concrete terms, this means, for example, that animal fats should be replaced by vegetable fats and that around half of the food consumed should consist of carbohydrates.
Fat should generally not make up more than 30% of the diet.
$config[ads_text1] not found

Eating habits
This important step is ultimately about applying what you have learned. E.g. Most people have certain rituals when buying food, according to which they buy certain things and not others.
There are also rituals, e.g. how a person a bread smeared.
This often does not work very consciously (ask yourself how many times in your life you have made bread for yourself), but is often "trained" over many years.
Aim of therapy must now be retrained this behavior. When you become aware of new foods (which are not so dissimilar to the "old" ones) if you have tried it, sooner or later you will certainly find some that are both tasty and lower in fat than the usual ones. It should be emphasized once again that it is not about bans (sweets are also allowed), It is about the responsible use of the knowledge that has been imparted to the patient about obesity.
It cannot be avoided to say that any weight loss efforts will be greatly enhanced by regular exercise.
Here, too, it is not about Olympic-level performance, but about the responsible handling of the knowledge imparted.
Every change in behavior, even small ones (e.g. small ways on foot and not by car, etc.) will have a lasting and positive effect on the patient. Here, too, it is important to set realistic goals, as there is otherwise the danger of destroying the motivation to continue the therapy.