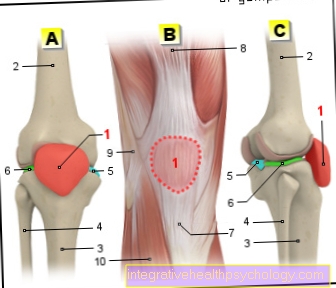
A quadriceps tendon rupture is a "disease" of the large thigh muscle on the front of the thigh. The quadriceps muscle itself is a muscle that consists of a total of four muscle bellies and is mainly responsible for flexion in the hip joint.
The muscle is attached to the kneecap and lower leg as well as to the hip bone with the help of tendons. A quadriceps tendon rupture is a tear in the tendons that attach the muscle. This tear can affect the entire tendon or just part of it.
Here you can find out everything about the quadriceps tendon

The causes of a tendon rupture can be broadly classified into two categories. On the one hand, tendon ruptures can occur as a result of sudden overloads or they can appear as a sign of fatigue. The main factor for the second variant is, on the one hand, the age of the patient or a disease of the tendon tissue in general.
Ruptures due to overuse often arise in connection with physical activity. Even if such injuries are much less common than other sports injuries, they can occur during intensive strength training.
$config[ads_text1] not found
A quadriceps tendon rupture in combination with an accident can either follow as a direct consequence of the accident, or the accident can create an overstrain, which as a consequence can lead to a rupture.
As a rule, the tendon of the quadriceps tears near the point of attachment on the kneecap or the lower leg. If the muscle is stretched slightly, a hard blow or entrapment can cause it to tear. If the tear has found a starting point on the tendon, this can spread across the tendon.
If, on the other hand, the accident leads to the lower leg being trapped and the remaining body weight is placed on the muscle strength of the quadriceps, the tendon can "tear" after prolonged stress.
A quadriceps tendon rupture is first and foremost a painful event. Since the tendon usually tears at its starting point on the kneecap, the pain is particularly intense here too. Furthermore, if the rupture is complete, the muscle tends to contract more than it would with a straight leg and flexed hip. The affected thigh appears thicker than the opposite side and you can see that the muscle belly has slipped upwards.
$config[ads_text2] not foundIf the tendon is only incompletely torn, you can feel a gap on the front of the thigh. Further symptoms are a decrease in strength when extending the leg or severe pain when trying to straighten the leg.
Find out more about the topic here: Pain in the thigh.
A dent in the actual muscle is unlikely to be found in a tendon rupture. Rather, it is a gap in the course of the tendon that can be identified when the tendon is felt. This is due to the fact that the muscle and thus also the tendon attached to it strive to contract. However, this gap only arises when the tendon is incompletely torn.
If, on the other hand, the tendon breaks completely, the entire muscle on the thigh slides up towards the hip. This causes the muscle to lose its elongated shape and take on a somewhat more rounded appearance.
A hematoma or bruise is always an indication that a blood vessel has been injured, from which the blood penetrates the tissue and is responsible for the formation of the hematoma. The bruise has the advantage that the accumulated blood will eventually be so much that it itself exerts pressure on the vascular injury and thereby stops the bleeding.
Since the muscle tendons and the muscle itself are also surrounded by blood vessels, a tendon rupture usually leads to the development of a hematoma. Since this is usually a major hemorrhage, the "breakdown" of the hematoma usually takes several weeks. It is therefore advisable to put pressure on the area as soon as possible after the rupture in order to limit the bleeding.
$config[ads_text3] not found
How do you treat a bruise? Read on here.
$config[ads_text2] not foundThe pain of a quadriceps tendon rupture is very impressive and probably of an almost unmistakable character. A previously existing heavy load on the quadriceps muscle leads to a sudden loss of strength, which is associated with a sharp, shooting pain.
As a rule, this pain then continues as a dull, pressing pain when a hematoma develops. When trying to straighten the knee again afterwards, sharp pain caused by the torn tendon can come back.
Also read the article: Front thigh pain.
A complete loss of function from an incomplete loss of function can also be distinguished from a loss of function. Since the quadriceps muscle is mainly responsible for knee extension and partly responsible for hip flexion, these movements are seen as functional tests for the muscle.
With a complete tendon rupture, the affected person is no longer able to straighten their knee. When trying to bend the hip against resistance, there is a noticeable reduction in strength on the affected side.
With a partial tear of the quadriceps tendon, however, there is a loss of strength when the knee is to be extended against a resistance at the shin. In hip flexion, on the other hand, there is hardly any reduction in strength with a partial tear.
An ultimately confirmed diagnosis for the attending physician is the MRI. This is able to map the soft tissue structures of the body so precisely that the torn tendon can be shown. In addition, it can be assumed that the previous medical history and physical examination will hardly allow any other option.
$config[ads_text4] not found
In addition to a typical situation caused by overstressing, there is a side-by-side comparison of the thigh and the patient's information on how the accident happened, as well as the sudden shooting pain and the resulting loss of function. A hematoma on the front of the thigh just above the knee also fits very well into the picture of a quadriceps tendon rupture.
These clues are usually sufficient as clues so that the MRI only serves as a final check.
As already indicated, the MRI of the thigh serves as evidence of the presence of a tendon rupture because it is able to depict soft tissue particularly well. Ruptures can thus be recognized very well.
Compared to the CT, there are two main advantages for the question of a tendon rupture. On the one hand, the MRI is able to show soft tissue in much greater detail, which is due to the imaging technology. While the CT works with X-rays and thus records the different densities of materials, the MRT works with a technology that is able to detect the different water content of matter. No X-ray radiation is needed, which is why the MRI produces virtually no radiation exposure for the human body.
The disadvantage of the MRI, however, is that the actual examination itself takes much longer. An examination of the thigh takes about 5 minutes.
During the examination, the person affected should keep their thighs as still as possible so as not to reduce the sharpness of the image.
More general information on the topic MRI can be found here.
Conservative treatment may be indicated for incomplete tendon ruptures. After the acute event, the patient is merely provided with painkillers and an attempt is made to remove the hematoma as quickly as possible. However, if there is a desire for increased physical activity, the incomplete rupture should also be treated surgically.
A complete rupture, on the other hand, is always treated surgically - the only exceptions here are people who can no longer be expected to undergo such an operation due to their state of health or people who do not necessarily depend on active extension of the knee. Those affected can then move their leg again. Although a reduction in strength is retained during knee extension, those affected can cope with their everyday lives normally and do not have a disturbed gait pattern.
$config[ads_text1] not foundAn orthosis is particularly important in the aftercare of a tendon rupture in order to avoid overstretching or overstressing the sutured tendon. An orthosis is a kind of guide cage for the knee joint. It extends across the thighs and lower legs and helps keep the knee at a fixed angle. This prevents the knee from bending too much, which could encourage a new rupture.
Depending on the orthosis model, the knee's flexion angle can be adjusted in order to gradually accustom the tendon to the flexion. The angle is then increased at weekly or bi-weekly intervals until approximately preoperative mobility is achieved.
A bandage can subsequently increase the stability of the knee somewhat. It can be worn during sports, for example, and, in addition to its light stabilizing effect, above all ensures that those affected have a feeling of protection - so it serves at least as much as a psychological protection factor.
More information on the subject Knee brace you'll find here.
Surgery is necessary for any complete quadriceps tendon rupture. It is the only way to give the muscle its function back. Depending on where the tendon is torn, different attachment points or surgical procedures are used.
However, surgery may also be indicated in the case of an incomplete quadriceps tendon rupture. This depends on the condition of the patient and the stresses to which the knee is to be exposed again after the operation.
The operation of the torn tendon should be carried out shortly after the rupture, as the two parts of the vision drift further and further apart with increasing time. The longer you wait, the more difficult the operation and the more unsatisfactory the result.
During the operation, the two tendon parts are sutured together again. In order to increase stability, the threads can, for example, be passed through specially made holes in the kneecap. Another way to gain additional stability is to use tendon material from your own body. For example, the semitendinosus muscle, which runs on the back of the thigh, can be used for this. Another possibility would be to use tendon material from the calf muscles.
Overall, the operation is a procedure that tends to be less complicated than other operations. Studies did not show any significant increases in infections or thromboses.
The follow-up treatment is very calm in the first few weeks after the operation or after the rupture. With the help of an orthosis or a splint, the knee joint is immobilized in order to give the tendon parts the opportunity to grow together again. As a rule, four weeks are recommended after an operation, and six weeks with conservative treatment.
Thereafter, with the help of physiotherapeutic support, you should slowly begin again to strain the muscles and the tendons.It is important to slowly get used to the knee again to the full range of motion and the full resilience and not to rush anything in this regard. Even after the operation, the tendon is still very prone to injury.
$config[ads_text2] not found
Find out more about the topic here: Knee brace.
As with all sports injuries, the healing time of a quadriceps tendon rupture depends to a large extent on the patient's cooperation. How much does he stick to the doctor's instructions; can he really wait long enough with the renewed exposure so as not to disturb the "growing together"?
Furthermore, the question arises what healing means in this context. Is it about the time until the tendon pieces have healed together again and one can carefully load the tendon again or does healing mean the establishment of perfect functionality, as before the tendon rupture.
With the first assumption, a duration of approx. 5 to 8 weeks can be assumed. It usually takes more than three months to reach the same state as before the injury.
This question is also difficult to answer across the board and is of course related to which sport is involved or the intensity with which it should be performed.
For sports with low stress on the thigh muscles, the rule is that these can be practiced again after approx. 3 months. For sports that put more strain on the thigh muscles, you have to slowly approach the strain again. Ideally, you can work together with a physiotherapist who can accompany the rehabilitation process.
Athletes with extreme strain on the thigh muscles would, however, be advised against continuing. These include, for example, weightlifters (who lift loads over 200 kilograms).