Duchenne muscular dystrophy, Duchenne disease;
engl. Duchenne’s disease, Duchenne Muscular Dystrophy
The Muscular dystrophy of the Duchenne type is next to the "myotonic dystrophy"the most common hereditary muscular dystrophy and shows a pronounced already in early childhood muscular dystrophy. The reason for this is a mutation in the genetic blueprint for an important structural protein of the muscle, des Dystrophins. Because of the inheritance, men are almost exclusively affected. The disease leads to progressive muscle wasting and weakness, progresses rapidly and ends fatally by infecting the respiratory and heart muscles. Those affected usually die in early adulthood.
$config[ads_text1] not found
Duchenne muscular dystrophy is one x-linked recessive hereditary diseasewhich, due to the absence or defect of dystrophin, an important structural protein in muscles, leads to progressive muscle wasting and sooner or later ends fatally.
Duchenne muscular dystrophy occurs at a frequency of about 1: 5000 die most common hereditary muscle disease of childhood. Due to the x-linked recessive inheritance, fmostly boys Affected by the full picture of the disease, girls only become ill if there is no intact blueprint for dystrophin on both X chromosomes, which is extremely rare.
In 2.5% of cases, carriers of a defective X chromosome show mild symptoms such as muscle pain, slight weakness or increased levels of a muscle enzyme (creatine kinase, CK) in the blood.
The symptoms of Duchenne muscular dystrophy usually show up before they reach school age.
The cause of the disease is the lack of the genetic blueprint for the Dystrophin protein on the X chromosome. As a rule, this is inherited, but a smaller part occurs spontaneously as a result of a random change in the parental genetic make-up.
In about 5% of the cases there is still a small residual production of dystrophin, which, however, is not sufficient to maintain muscle function and structure.
The lack of this important Structural protein of the muscle cell leads to instability of the muscle cell membrane ("muscle cell membrane") and increased membrane permeability. This allows harmful substances to penetrate the muscle cell unhindered, and important substances in the cell are also lost. Over time, the damage adds up and leads to progressive cell damage and cell death in the Muscles. This leads to the clinical picture of Duchenne muscular dystrophy. The lost muscle cells are partly replaced by fat cells, which in some parts of the body leads to an apparent enlargement of the affected muscles (Pseudohypertrophy).
The affected children usually fall through one delayed motor development (See also Medical check-up): They move little, learn to walk with a delay, fall frequently and are “clumsy”.
After learning to walk, the calves often increase in size considerably, the reason for this being the pseudohypertrophy of the calf muscles outlined above, the children also show Gait abnormalities in the sense of a Waddling gangs.
In the beginning, the disease primarily affects the Pelvic muscles, the children z. B. are unable to stand up from the supine position without the help of their arms. The maneuver instead, unconsciously carried out by the children, in which they turn in the prone position and rise above the quadruped position and support the arms on their own thighs "Gowers sign" called.
$config[ads_text2] not found
As the disease progresses, the abdominal and back muscles are increasingly affected, resulting in stronger and stronger ones Hollow back leads to the sick.
Accompanying it occur to varying degrees shortening and hardening of the Musculature on, which lead to additional movement restrictions v. a. in the hip, foot and knee joints. The muscle wasting in the shoulder region leads to protruding shoulder blades (Med .: Scapulae alatae, "angel wings"), the shrinkage of the neck muscles makes it difficult to straighten the head while lying down.
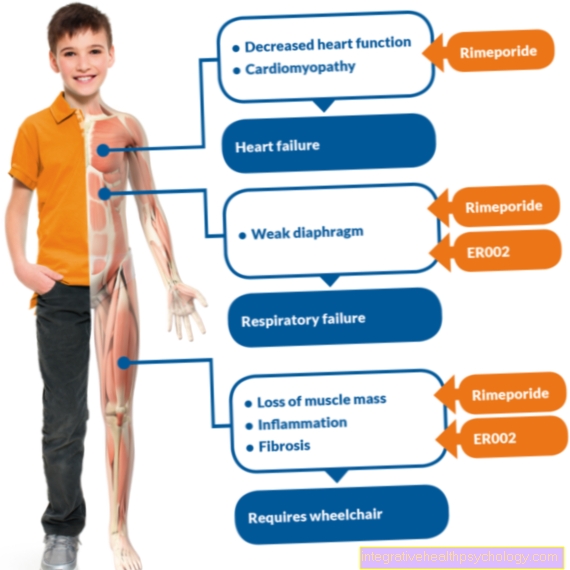
$config[ads_text3] not foundFrom around the age of 8 to 12, most patients are dependent on a wheelchair, and over time a spinal curvature often develops (Scoliosis) and deformation of the Rib cage. This and the ever advancing reduction of the Respiratory muscles lead over time to an increasingly restricted breathing capacity and u. U. to a serious risk to the patient. The restricted breathing, in turn, favors infections of the lung and the airways (see lung infection), which also threaten the patient. In the late stages of the disease, patients must be artificially ventilated.
In the process there will also be one Heart failure, due to it too Cardiac arrhythmias.
In about 1/3 of the cases there is also one intellectual impairmentwhich manifests itself in a learning disability.
The clinical picture and the course of Duchenne muscular dystrophy are in themselves very characteristic. A fundamentally similar disease mechanism shows the Becker or Becker-Kiener muscular dystrophy, which is to be distinguished from Duchenne dystrophy. In the Becker muscular dystrophy, the dystrophin protein is not absent, but it is present in a highly modified form so that it can only perform a residual function. The affected muscle parts are similar to those in Duchenne dystrophy, but the course is much slower and the severity less pronounced.
In principle, other reasons for delayed development come into question in the early stages, here are just one example of brain damage due to lack of oxygen or less birth called.
Due to the defect in the muscle cell membrane, the affected person shows one from birth strong increase in creatine kinase, an enzyme found in muscle, in the blood.
The neurological examination shows muscle weakness without sensory disturbances or muscle twitching, the reflexes are weak or have disappeared.
in the EMG (Electromyography) shows a typical picture for muscular dystrophies.
The human genetic examination of a blood sample can prove the defect in the genetic material, but this proof cannot be provided in approx. 30% of the cases.
In such cases, microscopic examination of a tissue sample allows for a Muscle biopsy (Sampling) the diagnosis by showing the lack of dystrophin in the muscle cell using a special staining method.
After the diagnosis it should heart be examined with ultrasound and EKG to detect damage early.
$config[ads_text4] not found
A causal therapy for Duchenne dystrophy is currently not possible, all hope lies in one future gene therapy. It is therefore important to ensure that those affected enjoy the highest possible quality of life for as long as possible by treating the symptoms.
These include, above all, massage, warm baths and measures to maintain automatic breathing for as long as possible (coughing exercises, singing, breathing training). Physiotherapy and training must be carried out very carefully so as not to damage the muscles through excessive strain, but they are useful to avoid stiffening.
There are various studies that investigate the possibility of having a beneficial effect on the course of Duchenne muscular dystrophy by administering drugs. This research is currently ongoing, so no general statements can be made at this point. Surgical measures can correct incorrect posture and improve movement restrictions.
In each case there is one genetic counseling to advise affected families, for example, to clarify the risk of developing other children. The connection to interest groups can help those affected to cope with life with the disease, to connect with other affected persons and to be informed about the current research.
The prognosis for the disease is still unfavorable: the average life expectancy of those affected is 20 to 40 years.











