laparoscopy
definition
Laparoscopy (laparoscopy) involves viewing the abdominal cavity using a video camera.
The video camera is inserted through a small hole in the abdominal cavity, usually the hole is made below the navel in order to view the organs of the abdominal cavity and the pelvis (especially the female pelvis in gynecology) from there.
Laparoscopy is not only popular in gynecology, but also in surgical operations, as the surgical field and thus the risk of infection can be kept very small. Thus, laparoscopy can be used for surgical purposes, i.e. as a treatment option, but is also of crucial importance for diagnostics.
method
Carrying out a laparoscopy always requires a certain amount of experience on the part of the doctor and should be carefully examined beforehand for advantages and disadvantages.
In laparoscopy there are also certain conditions that must be met.
For one thing, a patient is not allowed to fresh scars in the area of the abdomen or the upper pelvic area, on the other hand, there should not be too many older scars.
As with laparoscopy carbon dioxide (CO2) has to be pumped into the abdominal cavity and only through the breathing is eliminated, it is important that the patient receive a good to adequate Lung function Has. Patients with severe asthma or one chronic obstructive pulmonary disease are therefore often ruled out for a laparoscopic procedure.
Even patients with impaired heart function can often no longer be operated on laparoscopically as the risk of the CO2 unexpected complications occur in the abdominal cavity.
In order to perform a laparoscopy, the patient must be under general anesthetic be moved.
Only then can the doctor apply 3-4 stitches in the area of the abdominal wall, depending on which organ is diagnosed / treated.
The first stitch is usually there directly below of the navel. For one thing, this has optical Advantages since the scar is hardly noticed in this area; on the other hand, the position for the laparoscope is best here.
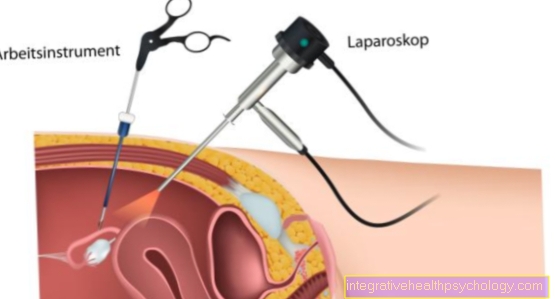
The laparoscope is one small camera, which also has a small lamp or Light source has to be able to display the area to be examined brighter, whereby the doctor can then follow the recordings of the camera via a screen. The laparoscope (which is a special one endoscope is introduced through the hole below the navel and from here, on the one hand, the organs of the abdominal cavity, i.e. Intestines, liver, Gallbladder and so on, on the other hand, the Fallopian tubes, the Ovaries and the uterus be examined in the woman.
Depending on which organs are to be viewed, the patient must be positioned differently.
When examining the Abdominal cavity lies the patient flat on the move.
When examining the female genital organs the patient also lies on the move, however, you will pool stored upwards so that the pool is highest. This has the consequence that all abdominal organs slide towards the chest and the female sexual organs are much better and more easily accessible and visible.
When the laparoscope is inserted through the abdominal wall into the abdominal cavity, the other necessary instruments (forceps, scissors ...) are also introduced into the abdominal cavity through 2-3 additional holes in the abdominal wall.
In order to get a better view of the area to be operated on or to be observed, the abdominal cavity is also used Carbon dioxide (CO2) inflated. For this, a small incision is made in the abdominal wall, through which a so-called special Insufflation cannula (Veres cannula ring) is inserted. This insufflation cannula is a kind of mini-tube through which the Co2 is pumped and which then through a so-called Trocar (also a kind of small tube) through which the video camera is then inserted.
Depending on Waist circumference and height of the patient can take up to 7l Co2 be pumped into the abdominal cavity.
This causes the abdomen to inflate enormously, so that the abdomen is tense during the entire operation, as in one pregnancy last month.
The advantage here is that it makes the field of view much larger and therefore much easier to use. In addition, the CO2 can be absorbed by the surrounding tissue and then exhaled through the lungs without causing any Complications or allergic reactions comes because CO2 is a natural substance in our body that the body is already familiar with. A so-called lift system is only used in rare cases, in which the abdominal wall is raised without CO2 in order to enlarge the operating room.
Is laparoscopy possible on an outpatient basis?
The hospital stay after a laparoscopy is already significantly shorter compared to surgery with an open abdomen.
A very short time after the procedure, the patient can get up again and take up everyday activities.
It is even possible to perform an outpatient laparoscopy. In this case, however, it is important that you have the Aftermath of anesthesia consider.
After such an intervention you are not able to actively participate in traffic, so you should have someone pick you up or take a taxi. Public transport can also be used, but is not a good option.
The use of heavy machinery should also only be resumed, at the earliest, one day after the procedure.
As a rule, however, after a laparoscopy, rest is required and you are still on sick leave for several days. In the case of outpatient procedures, you should still take sufficient care of yourself at home, do not lift heavily in the first few days and pay attention to the healing of the small wounds on the stomach.
The wounds are checked regularly by the family doctor in the first few days so that good healing is guaranteed and, in the event of inflammation, action can be taken at an early stage.
indication

When a laparoscopy is indicated depends entirely on the diagnosis or operation to be performed. As already mentioned, especially in gynecology, use is often made of laparoscopy to make a diagnosis which external palpation or through Ultrasonic is impossible to make out.
With the help of laparoscopy, the patency of the Fallopian tubes (Tuba uterina) examined, for example, if the desire to have children is unfulfilled.
This is done in the uterus (Uterus) given a dye, usually a so-called Contrast media. With the help of the video camera, you can now watch the migration of the dye from the uterus through the fallopian tubes.
If the fallopian tubes are continuous, this can be recognized by the problem-free color gradient, if they are not, you can see a stop of the color gradient somewhere.
In addition to diagnosing the fallopian tubes, endometriosis or cysts are also diagnosed using laparoscopy in gynecology.
In addition to diagnostics, laparoscopy is also used for treatment in gynecology.
On the one hand, in the case of an ectopic pregnancy in which the fertilized egg is implanted in the fallopian tube instead of in the uterus, it can be removed, and on the other hand, the fallopian tubes can also be severed.
A planned severing leads to the sterilization of the woman, which means that she will no longer be able to have children afterwards, although it should be noted that even sterilization does not lead to 100% safety and in rare cases a pregnancy can occur despite sterilization.
In addition to this drastic treatment method, a doctor can also take tissue samples, for example from the uterus, in order to determine whether a lump (tumor) may be present and whether it is more benign or more malignant.
Laparoscopy is not only very popular in gynecology.
Laparoscopy is also used more and more frequently in general surgery.
In many cases, laparoscopy is even part of the so-called gold standard, which means that laparoscopy is the first and best option. On the one hand, laparoscopy is used as an aid in making a diagnosis.
For example, biopsies, i.e. tissue sections, can be taken in order to determine whether, for example, a tumor is present.
Thus, laparoscopy is used when the findings are unclear, but it is also the method of choice for many operations. For example, in appendectomy, i.e. the removal of the appendix of the appendix, laparoscopy has now become the gold standard.
Laparoscopy is also the method of choice for the removal of the gallbladder (cholecystectomy), parts of the liver (partial liver resections) or parts of the intestine (for example iliozecal resection, sigma resection, rectal resection ...).
In addition, adhesions can occur in various areas of the gastrointestinal tract (gastrointestinal tract, GIT for short).
This means that individual sections of the intestine stick to one another and thus make the passage of food through the intestine considerably more difficult or impossible. These adhesions can then be removed by means of laparoscopy, the process known in medicine as adhesiolysis.
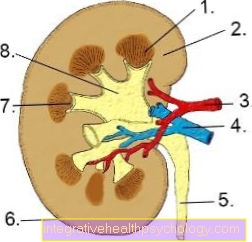
The spleen (splenectomy) or kidney (nephrectomy) can also be removed laparoscopically.
In addition, so-called hernias, i.e. protrusions of the intestine through the abdominal wall due to overpressure from the abdominal cavity, are treated with the help of laparoscopy, whereby a mesh is inserted at the appropriate point so that the intestine comes to rest regularly in the abdominal cavity and not through the Can turn the abdominal wall outwards.
A distinction is made between two techniques, on the one hand the TAAP (TransAbdominell PrePeritoneal) and on the other hand the TEP (Total ExtraPeritoneal).
The stomach can also be removed laparoscopically, often only removing parts of the stomach and not the entire stomach.
Indications for this are, for example, patients with food addiction who cannot reduce their weight without removing part of their stomach.
Laparoscopy can also be used as a therapy option for reflux disease; in addition, laparoscopy is used to sew over this area in a patient with an open (perforated) gastric ulcer (ulcer).
In addition to general surgery and gynecology, laparoscopy is also popular in urology. Here, laparoscopy is used to remove the prostate, for example, as this can lead to major problems such as urinary incontinence, the constant urge to urinate or cancer, especially in older patients. As already mentioned, the kidneys are also removed using laparoscopy. In addition, the ureter, which leads from the kidneys into the urinary bladder, can be straightened again using laparoscopy if there are any bottlenecks or bumps; this process is called ureteroplasty.
In general, it can be said that laparoscopy is being used more and more because the optical results after the operation are usually much more appealing and the risk of infection and the length of stay in hospital can be reduced.
Please also read our page on this topic Minimally Invasive Surgery.
advantages
Laparoscopy offers many advantages.
For one thing, there is cosmetic advantage. Instead of a big one scar Thanks to laparoscopy, there are only 3 or 4 small scars over the abdomen.
In addition to the cosmetic advantage, the small cuts also reduce that Risk of infection postoperatively.
In addition, compared to open surgery, laparoscopy is much gentler on the patient, which has the positive side effect that the patient no longer has to stay in hospital for a long time after the operation, but the patient can go inside 3-4 days back home and can fully exercise again after just a few weeks.
But laparoscopy is not only economically advantageous. Through the video recordings, certain sections can be enlarged and even the smallest angles can be made visible and any adhesions and the like can be removed. For the patient there is also the advantage that, on the one hand, the patient returns faster eat normally can, on the other hand, the patient usually has less pain.
disadvantage
However, laparoscopy does not only offer advantages. A disadvantage of laparoscopy is that the surgeon has the surgical field do not expand spontaneously can if the need arises.
On the other hand, the surgeon loses one of his most important tools, namely his sense of touch.
Also, like any other operation, others can organs, Vessels or annoy get hurt.
In addition, the general anesthetic As with all other operations, it can also lead to certain side effects and even intolerance. By pumping up the abdomen, there is also one after the operation Bloated stomach, occasionally too Pain or feeling unwell up to nausea. The risk of Bleeding, Thrombosis or Wound infections is quite small, but such side effects can occur.
All in all, however, the advantages of laparoscopy outweigh the advantages.
Complications of a laparoscopy
Compared to open abdominal surgery, laparoscopy is a low-risk procedure.
Nevertheless, this procedure also involves risks and complications can occur. There are initially the same risks as with other operations:
- Blood clots (Thrombosis, embolism, stroke, heart attack)
- Infections
- Bleeding
- Injuries to vessels
- Injuries to Nerven and surrounding Tissues and Organs
- as well as the Scarring.
The special complications can arise when introducing the Trocars arise. This happens without sight, so vessels and organs in the abdominal cavity can be injured.
This happens very rarely, however, as the surgeons proceed with caution. It may be necessary to enlarge the abdominal incision or to change the procedure and open the abdominal cavity with a large incision.
In addition, the abdominal cavity may already have adhesions before the procedure, from previous operations such as a caesarean section, or they may arise as a result of this procedure. Adhesions in the abdomen can also be painful.
The handling of the instruments during this procedure requires a lot of experience, which is why the aforementioned injuries to vessels, nerves and abdominal organs can occur.
In addition, pressure damage could result from positioning during the operation or from the instruments. Overall, however, it can be said that the risk of complications is lower with laparoscopic surgery than with open surgery.
Gas during a laparoscopy
During laparoscopy, several so-called trocars are inserted into the abdomen.
Before starting the laparoscopy, the gas carbon dioxide, or alternatively helium, is fed into the abdominal cavity via an access. This lifts the abdominal wall away from the organs and the surgeon has better visibility and working conditions during the operation, which further reduces the risk of injury to the patient.
The amount of insufflated gas depends on individual factors, such as the size of the abdomen for example.
Furthermore, the pressure in the abdomen is constantly measured during the procedure so that too much gas is not directed into the abdomen. Before the abdomen is closed after the end of the procedure, the gas is released again. It can happen that gas remains in the abdomen. But this is usually not a problem, because the body picks up the leftovers and they are over the lung exhaled.
Getting up early and moving around after the operation will help and alleviate possible discomfort. However, there are also laparoscopic procedures that can be performed without gas. The abdominal wall is raised mechanically. But they are less common than the gas variant.
Applications of laparoscopy
Gallbladder laparoscopy
The Gallbladder is responsible for many symptoms in the stomach.
Gallstones or the following sometimes Gallbladder infections are very painful clinical pictures that give the patient colicky pain.
It is therefore often necessary to remove the gallbladder. Also Gall bladders with polyps are removed to prevent degeneration into malignant cells.
The conventional surgical method with a large abdominal incision is only used today for complex inflammatory processes or major problems. Otherwise, today people like to use the laparoscopic procedure, in which the devices are introduced via 4 small incisions. The gall bladder is then mobilized from its location on the liver and removed under video view.
Since the gallbladder does not fit through the small openings, it is shredded in a bag in the abdomen or taken out through a larger incision.
This procedure is a very gentle procedure to remove the gallbladder relatively quickly and safely.
Laparoscopy of the appendix
The Removal of the appendix becomes necessary if this ignites (Appendicitis; med: Appendicitis). During this operation, too, the camera and working instruments are inserted into the abdominal cavity using the keyhole technique.
The appendix is found and displayed, the vessels supplying it must then be tied off or obliterated so that they do not cause bleeding, and then the appendix is separated.
The appendix is a small part that can easily be removed via the guide sleeve, i.e. an existing incision.
A drain is then inserted through which the wound secretion can flow out of the abdominal cavity and the patient can be discharged home for another 4-5 days.


.jpg)