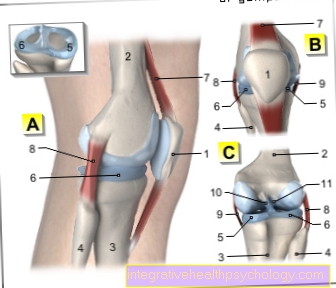
Articulatio genus, knee, thigh roll, tibial head, joint, femur, tibia, fibula, kneecap, meniscus, cruciate ligaments, anterior cruciate ligament, posterior cruciate ligament, collateral ligaments, inner ligament, outer ligament

A - Right knee joint from the left
B - Right knee joint from the front
C - Right knee joint from behind
You can find an overview of all Dr-Gumpert images at: medical illustrations
$config[ads_text1] not found
The Knee joint is the largest and most stressed joint of the human body. Accordingly, the knee is also the most commonly injured joint.
At the Knee joint it is a so-called rotary hinge joint. This means that the knee joint can be bent as well as rotated
The knee joint is made up of three bone formed, the Thigh bone (femur), the Shinbone (tibia) and the Kneecap (patella). The Fibula is not involved in the knee joint.
$config[ads_text2] not found
The knee joint is differentiated into two lower joints:
The Thigh - shin - joint
The joint is formed by the thigh bone with its two joint heads (medial and lateral femoral condyle) and the tibial plateau (tibial plateau). The round heads of the thighs lie in the small hollows of the tibia plateau (intercondylar fossa). The ratio of the joint surface of the thigh to the shin is about 3: 1.
Since there is only a point-like contact between the thigh and the shin, the diffraction of the knee joint to a rolling sliding movement.
The Thigh - kneecap - joint
When you bend, the kneecap slides through a predetermined slideway between the thighbone heads (femoral condyles). Overall, the kneecap can slide between 5 - 10 cm. In order to be able to cover this distance, larger sliding layers are necessary. For this purpose, two bursa (prepatellar bursa and infrapatellar bursa) form two large sliding gaps. The large thigh muscles (Musculus quadrices femoris) attach to the kneecap (patella) from above. The strength of these muscles is about the Kneecap (Patella) diverted to the lower leg. The kneecap tendon (patellar tendon) attaches to the lower kneecap pole, pulling towards the front edge of the tibia and connecting to the tibia at a protruding bone (apophysis = tibial tuberosity).
$config[ads_text3] not found
There are various knee stabilizers to stabilize the thigh in the small socket of the tibia (intercondylar fossa):
The menisci (plural of the meniscus) help with the transmission of force from the thigh to the lower leg. Since the head of the femur is round and the tibia plateau is almost straight, there is only point contact. To increase the contact area, there is the Medial meniscus and the External meniscus. They are inserted on the inside and outside as a kind of shock absorber and help to distribute the force more evenly. You can find more about this in our articles Meniscus and Meniscal lesion (Meniscus damage).
The cruciate ligaments prevent the femoral heads from sliding forward in relation to the shin (anterior cruciate ligament) or to the rear (posterior cruciate ligament). They are the decisive stabilizers of the knee joint.
The collateral ligaments stabilize in a lateral direction so that the knee joint is prevented from buckling into a bow-leg or knock-kneel malposition. The inner ligament is firmly fused with the inner meniscus, so the inner meniscus is more immobile than the outer meniscus.
The joint capsule of the knee joint is very tense and stabilized when it is fully extended. With increasing flexion it slackens and the remaining stabilizers have to take over the tasks.

$config[ads_text4] not found
Normally the knee can be bent to 120 - 150 ° and, depending on the ligamentous apparatus, about 5 - 10 ° overstretched. With 90 ° flexion, the knee can be rotated approximately 40 ° outwards and 10-20 ° inwards.
The knee joint must bear the entire load of the trunk on the lower leg (Shin = Tibia).

taken from the front (a.p.)

No joint in the human body has more injuries than the knee joint.
The most common disease of the knee joint is Osteoarthritis of the knee. This results in damage to the cartilage sliding layer of the knee joint. Can follow inflammation, Pain, restricted mobility and instability.
Further information can be found under our topic:
In addition to the cartilage damage, this occurs particularly with increasing age Tears in the meniscus more often before. Due to the lack of healing potential of the meniscus, only a partial removal of the torn meniscus remains, apart from a few exceptional cases.
Further information can be found under our topics:
One is less common, but usually more serious Cruciate ligament injury, as you significantly reduce the stability of the knee joint. In comparison, the anterior cruciate ligament injury is more common than the posterior one.
Further information can be found under our topic:
Torn collateral ligaments often occur in combination with other injuries. While inner ligament damage has good healing potential, it must be complete Outer ligament tears are usually treated surgically.
Further information on the subject can be found at: Inner ligament stretch in the knee
Knee joint pain can have various causes.
Depending on the localization of the pain, this can occur different diseases or injuries Clues.
Also the point in time at which the pain preferentially occurs (at rest, at night, as initial pain, during exertion), can provide further clues as to the underlying cause.
Internal knee pain:
Knee pain, mostly on the inside of the knee, is often indicative of one Meniscus damage down.
Especially the one Medial meniscus is often injured in many sports injuries. This can be noticeable by pain on the inside of the knee.
Also one Leg malposition (If one) can lead to permanent damage to the inner meniscus, as the pressure on it is increased by the uneven load. Ultimately, this can result in a Osteoarthritis in the knee joint train, which can express itself through internal knee pain.
Ultimately, a Bursitis or a muscular damage that cause discomfort.
External knee pain:
Pain on the outside of the knee can also be caused by a Leg malposition (X-leg) be conditional. In this case, the external meniscus is stressed more than normal.
This can damage the meniscus in the long term and, as a result, become a Osteoarthritis development to lead. This can be responsible for the pain.
Another cause of outside knee pain is one Damage to the hamstring tendon (Biceps femoris).
Knee pain on the outside of the knee that occurs in runners can also be attributed to the so-called Runner's knees indicate a pain syndrome caused by the Overuse of the iliotibial band, a fascia band on the outside of the thigh.
The symptoms typically only occur when running, and later when walking.
Front knee pain:
Pain that is mainly felt in the front area of the knee can be attributed to a Damage to the patella tendon Clues.
Also one Malformation of the kneecap (Patellar dysplasia) can cause these complaints, as in this case the kneecap does not fit optimally into its abutment and can cause pain due to friction and incorrect loading.
A Bursitis of the knee can also cause pain in the anterior knee area.
Back knee pain:
Pain in the hollow of the knee can have multiple causes. These include vascular, bone and nerve damage, ligament or meniscus injuries, as well as one Baker's cyst.
This is an outgrowth of the joint capsule of the knee joint that is enlarged by Synovial fluid arises. The production of synovial fluid is often significantly increased due to chronic inflammatory processes, for example in the context of a rheumatic disease.
When a Baker's cyst rips, it can become a dangerous one Compartment syndrome come.
Generalized knee pain:
If the pain is diffuse throughout the knee joint, it may be a inflammation, one rheumatic or one degenerative disease (arthrosis) act.
The knee joint is common in parallel to an inflammatory process swollen, overheated and if necessary reddened.
Especially Start-up pain and Stiffness after a longer period of rest, this can speak for knee osteoarthritis.
For systemic signs of inflammation, such as fever or poor general condition it is more likely that it is an acute inflammatory process.
In any case, a visit to a doctor is advisable if the complaints persist.

Who am I?
My name is dr. Nicolas Gumpert. I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me live every 6 weeks on "Hallo Hessen".
But now enough is indicated ;-)
The knee joint is one of the most stressful joints.
Therefore, the treatment of the knee joint (e.g. meniscus tear, cartilage damage, cruciate ligament damage, runner's knee, etc.) requires a lot of experience.
I treat a wide variety of knee diseases in a conservative way.
The aim of all treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
You can find more information about me at Dr. Nicolas Gumpert
To stabilize the knee joint, it can be helpful to put tape around it. This method is particularly useful for follow-up treatment after knee injuries, as the tape movement supportive works, but does not restrict movement.
In addition, it has one pain relieving effect and gently restores the knee to its normal functionality.
There are a few things to consider when taping the knee joint. First of all, the tapes tailored become. It will two shorter ones and two longer strips needed.
To measure the optimal length, use the Kneecap. The shorter tapes should end about three fingers wide above and below the kneecap, the two longer tapes about six fingers wide, i.e. three fingers wider than the shorter tapes.
Then the knee is reduced by about Bent 70 ° and the shorter tapes are glued tightly around the kneecap. It must full train be applied to the tapes, but do not pull the skin when sticking them, otherwise blisters may form; so always make sure that the ends of the tape are loosely attached to the skin.
Then the longer tapes glued. These will NOT under tension but loosely glued to the knee next to the shorter inner tape strips. The strips should overlap about a finger's breadth.
When the knee is then moved, the skin over the kneecap should wrinkle significantly in the extended position. The tape shouldn't feel uncomfortable.Overall, it is important to note that the inner strips are glued tight enough around the kneecap and the outer strips are applied around them completely without tension. This is the only way for the kinesiotape to develop its optimal stabilizing effect.
Read more on this topic at: Tap your knees
An operation on the knee joint can be necessary in the event of various damage or diseases of the knee joint, if conservative therapeutic measures have not been successful.
Meniscus operations:
A meniscus injury can occur as part of sports accidents.
If the meniscus is torn, it is often necessary to remove it to sew. However, this only works for not too large cracks and tears in a well-perfused area of the meniscus, as otherwise the healing may not proceed adequately.
In such cases, the torn part of the meniscus removed and be replaced by synthetic or natural material (Meniscus transplant).
Cruciate ligament surgery:
Cruciate ligament injuries also often have to be operated on.
A torn cruciate ligament leads to instability of the knee joint and can lead to the development of consequential damage and a Osteoarthritis of the knee to lead.
The standard procedure nowadays is autologous transplant an endogenous tendon to replace the injured cruciate ligament. This is usually done using the tendon of the Semitendinosus muscle used.
Is the cruciate ligament with a piece of bone torn off, this piece of bone, including the cruciate ligament, can be returned to its original position screwed become. This is particularly common in children and adolescents. An autologous transplant is then not necessary.
Same goes for one only torn cruciate ligament. This can often be reconstructed and sutured without the need for additional tendon tissue.
Cartilage transplant:
There is a new treatment concept for cartilage damage in the knee joint. Be there The body's own cartilage cells are taken, bred and secondarily transplanted back into the knee jointwhere the cells can grow and compensate for cartilage defects.
Knee prosthesis:
Especially in the context of a serious one Osteoarthritis of the knee In the long run, irreversible damage to the joint can occur, so that normal function is no longer possible.
If all conservative treatment measures have been exhausted, the last resort can be a Knee endoprosthesis (Knee replacement) can be used. The knee joint is completely through artificial material replaced.
This is followed by a intensive physiotherapyso that the new knee joint is optimally resilient and the body can get used to it.
Lateral retinaculum split:
This procedure on the knee joint is performed when a Misalignment of the kneecap is present.
In this case, the kneecap is pulled too much outward by the ligamentous apparatus and thus leads to an increased pressure load on the outer joint part. In the long run, this can cause consequential damage.
By a Splitting of part of the lateral ligamentous apparatus, the lateral retinaculum, the tension on the kneecap is reduced so that it is shifted more towards the center.
This distributes the force more evenly across the knee joint.
Kneecap surgery:
The so-called kneecap surgery according to Blauth is used when the lateral splitting of the retinaculum has not improved the symptoms.
The aim here is that the kneecap is shifted more towards the center and the pressure can be distributed more evenly on the joint.
To do this, the Patellar tendon severed and shifted further inwardsso that the kneecap is pulled towards the center.
The knee joint is a compound joint. On the one hand, it consists of the Kneecap joint (Femoropatellar joint) and on the other hand from the Popliteal joint (Femorotibial joint).
The popliteal joint is the actual knee joint, which enables flexion in the knee. Again, it's a combination of one Hinge- and one Wheel joint and is therefore also called Swivel joint designated.
Movements that can be executed accordingly are one Elongation and diffraction, as well as one in the bent state Outside- and Internal rotation of the knee.
The kneecap joint is also called Slide joint referred to because the kneecap only slides in a bony groove at the lower end of the thighbone. It is held in place by ligaments and slips over the cartilaginous joint surface when the knees are bent and stretched.
Since the knee joint is exposed to great stress, it needs additional stabilizers.
Hence it is with the front and posterior cruciate ligament, as well as the Outside- and the Medial meniscus fitted. The menisci buffer shocks and ensure a more stable connection between the upper and lower legs.
So that the knee joint can withstand daily loads, it is stabilized by numerous ligaments. Depending on their location, these are divided into a front, rear, side and central group. The ligaments are often damaged in sports injuries.
Front ligaments:
The front ligaments include that Kneecap ligament (Patellar ligament) and the Retinaculum patellae.
The kneecap ligament connects the kneecap to the front surface of the tibia. It is therefore very important for the transmission of force from the upper to the lower leg as part of the stretching movement in the leg.
The patellar retinaculum lies to the side of the kneecap and secures it in place. In addition, with its various proportions, it is part of the Joint capsule of the knee joint.
Back ligaments:
At the back of the knee there are two more ligaments that stabilize the knee joint, on the one hand that sloping back of the knee (Ligamentum popliteum obliquum) and on the other hand that arched popliteal ligament (Arcuate poplite ligament). They are also part of the joint capsule.
Side bands:
The lateral ligaments of the knee joint are also called Collateral ligaments designated.
The inner collateral ligament runs inside the knee (Tibial collateral ligament), the outer collateral ligament runs on the outside of the knee (Ligamentum collaterale fibulare).
They stabilize the knee especially in the Stretched positionbecause they are relaxed when the knee is bent. This prevents the knee from slipping sideways when the knee is extended.
The bands work one O- or X-leg deformity opposite. It is important that that The inner ligament is firmly fused with the joint capsule and the inner meniscus is, while the outer ligament has no fixed connection to the joint capsule or the outer meniscus.
Therefore, if the inner ligament is injured, the medial meniscus is often also injured. If the anterior cruciate ligament is also injured at the same time, one speaks of a "unhappy triad“.
Central bands:
The two cruciate ligaments (Ligamentum cruciatum anterius and posterius) educate the central tape backup of the knee joint. They cross over between the upper and lower leg bones.
Their position stabilizes the knee in the frontal plane, thus preventing the bones from sliding back and forth against each other. They also inhibit internal rotation (Inward rotation) of the leg.
Inflammation of the knee joint can have different causes. For example, it can be caused by an injury Wear processes (degeneration), by a Autoimmune disease or by a Infection with pathogens caused.
Ultimately it comes to one Inflammatory response in the knee joint, which is through a swelling, overheat, Redness and Pain expresses. As a result, the function of the knee joint is often significantly restricted.
Especially at bacterial infections of the knee can have symptoms like general feeling of illness and fever to be added.
To determine the exact cause of knee inflammation, the Joint effusion to be punctured. The fluid is withdrawn from the knee joint with a cannula and can then be examined for possible pathogens.
The problem with inflammation of the knee joint is that it can cause permanent damage to the joint. The cartilage in particular is attacked by the inflammatory reaction.
Has the damage progressed so far that Painkiller and anti-inflammatory drugs can no longer provide relief and other joint-preserving measures do not bring any improvement, the replacement of the knee joint with a prosthesis should be considered.
For this reason, knee pain that persists over a longer period of time should always be clarified by a doctor. In this way, suitable therapy can be initiated at an early stage and long-term damage can be avoided.
Bursa are used for Cushioning of mechanical stress, as well as improving the gliding ability of tendons and ligaments.
There are several bursae in the knee area, as the knee is heavily used every day and it can be relieved in this way. A large bursa (Prepatellar bursa) is located between the kneecap and the overlying skin.
She serves the The ability of the skin to slide on the kneecap when flexed of the knee. The suprapatellar bursa is also known as the suprapatellar recess. It is another bursa and lies between the lower end of the thigh bone and the Quadriceps tendon.
This will make that smooth gliding of the tendon over the bone when flexed of the knee. Finally, the infrapatellar bursa lies under the patellar tendon and allows it to slide on the tibia when the knee is flexed.
The bursa can become infected with an injury, wear and tear, or infection bacteria, Viruses or Mushrooms ignite and become one painful swelling of the joints With Redness, overheat and Function restriction to lead.
If you have symptoms that indicate bursitis, a doctor should be consulted in order to avoid possible consequential damage to the joint.
Also read more on the topic: Bursitis on the knee












