Medical: Vesica biliaris, Vesica fillea
Bile, gallbladder duct, gallbladder inflammation, porcelain gallbladder
English: gall bladder
Also read our topic: Gallbladder Inflammation
The gall bladder is a small hollow organ with a capacity of about 70 ml, which is located on the underside of the liver in the right upper abdomen. The task of the gallbladder is to store the bile that is continuously formed by the liver between meals and, if necessary, to release it into the duodenum for digestion.

You can find an overview of all Dr-Gumpert images at: medical illustrations
$config[ads_text1] not found
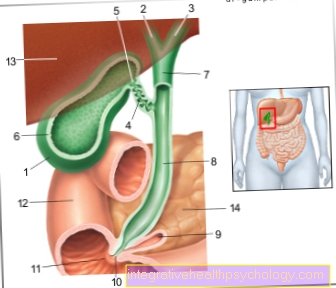
The gallbladder serves the Storage of the bilethat of the liver is produced. Accordingly, it is in the immediate vicinity of the liver right upper abdomen under the right costal arch. There it is with the bottom of the right lobe of the liver grown together and thus fixed in their position.
The gallbladder is about 6-10cm long and 4cm wide. Your neck opens into the Cystic duct, the Gallbladder duct. This in turn is with the Common hepatic duct, the Bile duct of the liver connected.
From the point where both gears merge, the corridor is also called Common bile duct designated. This finally flows together with the passage of the pancreas in the Duodenum and enables the bile to be released as part of the digestive process. Is the gallbladder ignited or otherwise ill, this can cause pain in the due to their anatomical position right upper abdomen to lead.
The Gallbladder like most abdominal organs, lies within the peritoneum (Peritoneum). It is on its top and back with the liver grown together. On the lower and front sides, the gallbladder is in contact with the duodenal bulb (transition stomach - duodenum), the pancreas (Pancreas) and the Colon transversum (part of the Large intestine).
$config[ads_text2] not foundThe gallbladder is divided into different sections: pit (fundus), body (corpus) and as (cervix). The pit and body of the gallbladder are the parts that make up the Bile (Bile) save. The neck of the gallbladder continues to taper until it finally merges into the gallbladder duct (ductus cysticus).
The blood supply is mainly provided by the gallbladder artery (arteria cystica), which branches off from the hepatic artery (A. hepatica propria).
In addition, individual small vessels from the liver supply parts of the gallbladder. The venous (low-oxygen) blood flows through the portal vein into the liver. This is why gallbladder cancer often causes metastases (daughter tumors) in the liver.


Histologically, the wall of the gallbladder consists of three layers: from the inside to the outside
The mucous membrane of the gallbladder consists of a single layer of covering tissue (epithelium) and is heavily folded when at rest. This allows the mucous membrane to expand easily when stretched.
On the inside, the mucous membrane cells are marked by a so-called brush border. This brush border consists of countless small protrusions of the mucous membrane cells to enlarge the surface.
This is important because most of the time the superficial cells actively try to draw water from the bile. They do this by using special proteins to transport salt out of the liquid, which is then followed by the water.
$config[ads_text2] not found
$config[ads_text3] not foundThe muscular layer of the gallbladder is made up of smooth muscle that extends around the gallbladder. When it becomes tense, the stored bile is squeezed out.
The tension is partly triggered by nervous impulses; The most important signal, however, is the hormone cholecystokinin from certain cells of the gastrointestinal tract.
The connective tissue layer (advdentitia) of the gallbladder is created by growing together with the inner layer of the peritoneum (peritoneum). As a result, the gallbladder is mobile, but inflammation can easily spread to the very pain-sensitive peritoneum (peritonitis).
The job of the gallbladder is to Storage and processing of the bile produced in the liver.
The gallbladder forms the end point of the Gallbladder duct (Cystic duct)through which the gallbladder connects to the Liver-bile duct (ductus hepaticus) connected is. From the point at which the two corridors join, one speaks of Common bile duct, the common bile duct. This bile duct finally unites shortly before its mouth with the excretory duct of the Pancreas (pancreas).
The opening into the small intestine is a constriction with a sphincter muscle (Papilla Vateri, Papilla duodeni major). This sphincter muscle is always tense and closes the exit of the bile duct. This means that the bile ("bile") cannot drain away, which in turn leads to an intentional congestion of the bile into the gallbladder. The bile is now temporarily stored in the gallbladder until we eat food.
The digestive process leads, among other things, to the fact that the sphincter muscle relaxes and releases the opening in the duodenum. Now there is rhythmic tension in the muscles (contractions) in the gallbladder and in the gallbladder duct (triggered by the hormone Cholecystokinin). These contractions cause the stored in the gallbladder bile active in the Small intestine is transported out. In the small intestine, the bile is needed for fat digestion and is used to eliminate poorly soluble substances from the body.
$config[ads_text4] not found
So that the gall bladder does not threaten to burst due to too much fluid at some point, pure water and common salt (NaCl) are removed from the stored bile. This means that the volume is reduced to up to a tenth of the original amount of fluid and consequently the concentration of the individual substances in the bile increases significantly. This increases the likelihood that it will lead to the formation of Gallstones comes.
Pain in the area of the gallbladder can be attributed to different causes. Often there is one Inflammation of the gallbladder, one acute cholecystitis in front. This can for example by Gallstones to be triggered.
Other causes of inflammation of the gallbladder include, for example Bacterial infections, Injuries to the abdominal organs, Tumors or Malformations the gallbladder / bile duct.
In case of acute inflammation of the gallbladder, the area is under the right costal arch very painful on pressure. Also to cough can cause severe pain. Sometimes additional symptoms such as fever, chills, nausea and Vomit on.
The cause of the gallbladder infection lies in one Stone sufferingso can be a characteristic colicky pain occur, which sets in acutely and violently and manifests itself in convulsive waves. These are caused by muscle contractions in the gallbladder and bile duct, which are intended to drive stones out.
Gallstones, which are responsible for pain in the gallbladder area, are often associated with nausea and a feeling of fullness - especially after very high-fat meals.
Will be a acute Inflammation of the gallbladder chronicso the pain changes too. They are usually weaker, but mostly exist throughout. Due to the chronic inflammation, the gallbladder can become a so-called Porcelain gall bladder develop. This is characterized by a thickened wall with calcium deposits. It can become malignant and must be surgically removed.
Also Gallbladder cancer can cause gallbladder pain, but this does not occur until the disease is advanced. Initially, the disease presents very few symptoms.
It is not uncommon for pain that is actually caused by stomach going out, confused with gallbladder pain. An easy one Inflammation of the stomach lining can through pain im right upper abdomen perceived and falsely projected onto the gallbladder. Last but not least, muscular or neural causes can also cause pain in the gallbladder area. The gallbladder itself is not always the place of origin of the symptoms.
$config[ads_text1] not foundDue to the various causes of the pain, a doctor should be consulted if there is no improvement.
Since there are numerous, poorly water-soluble substances in the bile, the risk of crystallization is increased. In order to prevent stone formation, it is necessary that the individual components of the bile fluid are in the correct ratio to one another.
Often a high cholesterol level (cholesterol) in the blood and thus also in the bile this relationship is disturbed and the formation of Gallstones. In most cases (> 60%) the person concerned does not even notice this (silent stones).
Only when this gallstone blocks drainage channels (Cholestasis), reflexes occur Convulsions of the muscles and too sudden, very strong colicky painwhich are usually located on the right upper abdomen, but can also radiate into the right shoulder. The occlusion of the biliary tract leads to two problems:
Further information is available under our topic:
Inflammation of the gallbladder (Cholecystitis) is a complication of gallbladder stone disease (cholel cystolithiasis).
Blocking the single inflow or outflow creates an environment in the gallbladder that ultimately leads to an inflammatory reaction in the gallbladder.
This inflammation leads to a Thickening of the gallbladder wall immigrated inflammatory cells (white blood cells: lymphocytes and granulocytes), a greatly increased sensitivity to pain and possibly systemic complications such as fever, chills, Formation of acute phase proteins (CRP).
For bacteria, the constellation of a cavity (here: the gall bladder) without direct contact with the outside world (as a stone blocks the drainage) creates excellent growth conditions.
Individual bacteria of the normal flora of the intestine (mainly Enterobacteriaceae and Enterococci) can then multiply almost undisturbed in the gallbladder and one purulent inflammation trigger (gallbladder empyema).
This is very dangerous as the bacteria are a Blood poisoning (sepsis) and are often resistant (insensitive) to numerous common antibiotics (drugs that kill bacteria).
$config[ads_text2] not found
Therapy usually consists of surgical removal of the gallbladder (cholecystectomy).
You can find more information on the topic here: Inflammation of the gallbladder
Gallbladder cancer is rather rare (5 cases per year / 100,000 patients.
For comparison: lung cancer 60 cases per year / 100,000 patients; Lung cancer) but very malicious cancer.
Cancer is caused by an accumulation of genetic mutations (changes in genetic information).
These are risk factors Gallstone disease / Gallstones (Cholecystolithiasis) and inflammation of the gallbladder (cholecystitis), although there is still no evidence of a direct causal relationship.
The problem with gallbladder cancer is the lack of typical symptoms in the early stages of its development. The cancer is usually only discovered when it has already spread (metastasized) via the lymphatic or bloodstream. In such cases the prognosis is very bad. Symptoms are possible but very unspecific Jaundice (jaundice), Biliary colic, Weight loss or diffuse pain, especially in the upper abdominal region.
You can find more information on the topic here: Gallbladder cancer
Gallbladder polyps are called benign tumorsthat can form in the gallbladder wall. Most of time are these growths symptomless and are only at random sonographic Investigations (ultrasound) discovered. Symptoms include pain in the upper right abdomen, nausea, and indigestion.
The causes of polyp formation can be varied. One possibility is that a diet high in cholesterol increases the cholesterol content of the bile. The excess cholesterol is then either deposited on the gallbladder wall (Cholesteatosis) or deposits of cholesterol form in the mucous membrane, which lead to bulges. This form of the tumor is too Cholesterol polyps called.
Other options are Growths of the mucous membrane and of the glandular tissue the gallbladder wall, also known as polyps.
The The risk of degeneration from gallbladder polyps is very low. In the case of 1 cm tumors or particularly rapid growth, the entire gallbladder (Cholecytectomy) recommended.
If the blood flow through the liver is slowed by damage to the liver tissue (e.g. Cirrhosis of the liver), the blood backs up into the portal vein.
The resulting increase in blood pressure is called Portal hypertension. We are now looking for other ways (the portacaval anastomoses) to re-enter the blood past the liver heart to transport back.
Further information is available under our topic: Portal hypertension

The removal of the gallbladder is medically called Cholecystectomy designated. Since a person can live without a gallbladder, the operation does not usually cause any major impairment for the patient. The procedure is indicated for various diseases and should then be carried out.
Read more about gallbladder removal here.
Indications for gallbladder removal:
The gallbladder is removed if the patient has gallstones, develops biliary colic due to a stone discharge in the bile duct, or if the gallbladder is badly inflamed.
Chronic inflammation of the gallbladder can cause a Porcelain gall bladder develop which has a thickened and consolidated wall. This can later degenerate and lead to gallbladder cancer, so a Porcelain gall bladder also removed.
Another indication for removal are polyps in the gallbladder, as these can also become malignant. The same applies, of course, to existing gallbladder cancer. Is the bile duct of the gallbladder (Cystic duct) and this leads to a build-up of the bile, the gallbladder must often be removed in this case.
Surgical procedure:
There are several methods that can be used to remove the gallbladder. Usually one will laparoscopic gallbladder removal made, which means that no large abdominal incision is required. Alternatively, the gallbladder can also be used as part of a open surgery, that is, can be removed through a large abdominal incision.
Laparoscopic Cholecystectomy:
The patient is placed under general anesthesia for the laparoscopic removal of the gallbladder. Then the various access routes are opened.
To do this, a small skin incision is made directly above or below the navel, below the breastbone and to the right of the navel, through which an instrument can then be inserted into the body.
The laparoscope with the camera is inserted through the access at the navel. In this way, the surgeon can see exactly where he is on a screen. In addition, the stomach is filled with carbon dioxide (CO2) inflated so that the view of the gallbladder and surrounding structures is easier.
The cutting and gripping tools are brought in through the other entrances. Finally, the gallbladder is detached from its bed on the liver and in a so-called Recovery bag wrapped. This ensures that during the subsequent removal - mostly through the access at the navel - the entire gallbladder is pulled out and no piece of tissue is lost.
Once the gallbladder has been removed, wound drainage can be placed so that the wound secretion and blood can drain off for a while after the operation. The drain will be removed later. The small skin incisions are closed again with a few stitches and the stitches are pulled after a few days. Later, only small, inconspicuous scars from the operation usually remain.
Single port operation:
The so-called single-port operation is a variant of the laparoscopic gallbladder removal Only a single access is required in the area of the navel, which is why no visible scars remain after the operation. The SILS technique is used for this procedure (Single Incision Laparoscopic Surgery).
The surgeon inserts a special, articulated instrument through the access at the navel into the abdomen. With this, the gallbladder can be removed as with the conventional laparoscopic variant and pulled out through the navel.
Open surgical cholecystectomy:
The open variant of gallbladder removal is also performed under general anesthesia. An approximately 10cm long skin incision is made in the area of the right costal arch through which the surgeon can access the gallbladder bed. There the gallbladder is exposed and can then be removed. As soon as bleeding vessels are closed, the surgical area can be closed again with sutures.
This method is used in particular when the removal of the gallbladder is more complicated, for example in the case of strong adhesions between the gallbladder and surrounding tissue or large collections of pus.
Advantages and disadvantages:
The procedure by which the gallbladder is removed is selected based on the patient and health circumstances. The advantage of laparoscopic removal is the lower burden on the organism and circulation, the smaller wound area and the more inconspicuous, shorter scars that remain after the operation. In addition, after the procedure, the patients are more mobile and able to regain strength than with the open surgical method. The single-port technique in particular delivers a cosmetically good result, as the scar in the navel cannot be recognized as such.
The open surgical variant is still to be selected in more complicated cases, as the surgeon can then recover the gallbladder more safely in this way without possibly damaging neighboring structures.












